Spinal Cord Stimula
Spinal cord stimulation is a neuromodulation treatment that may help selected patients manage chronic nerve-related pain signals.
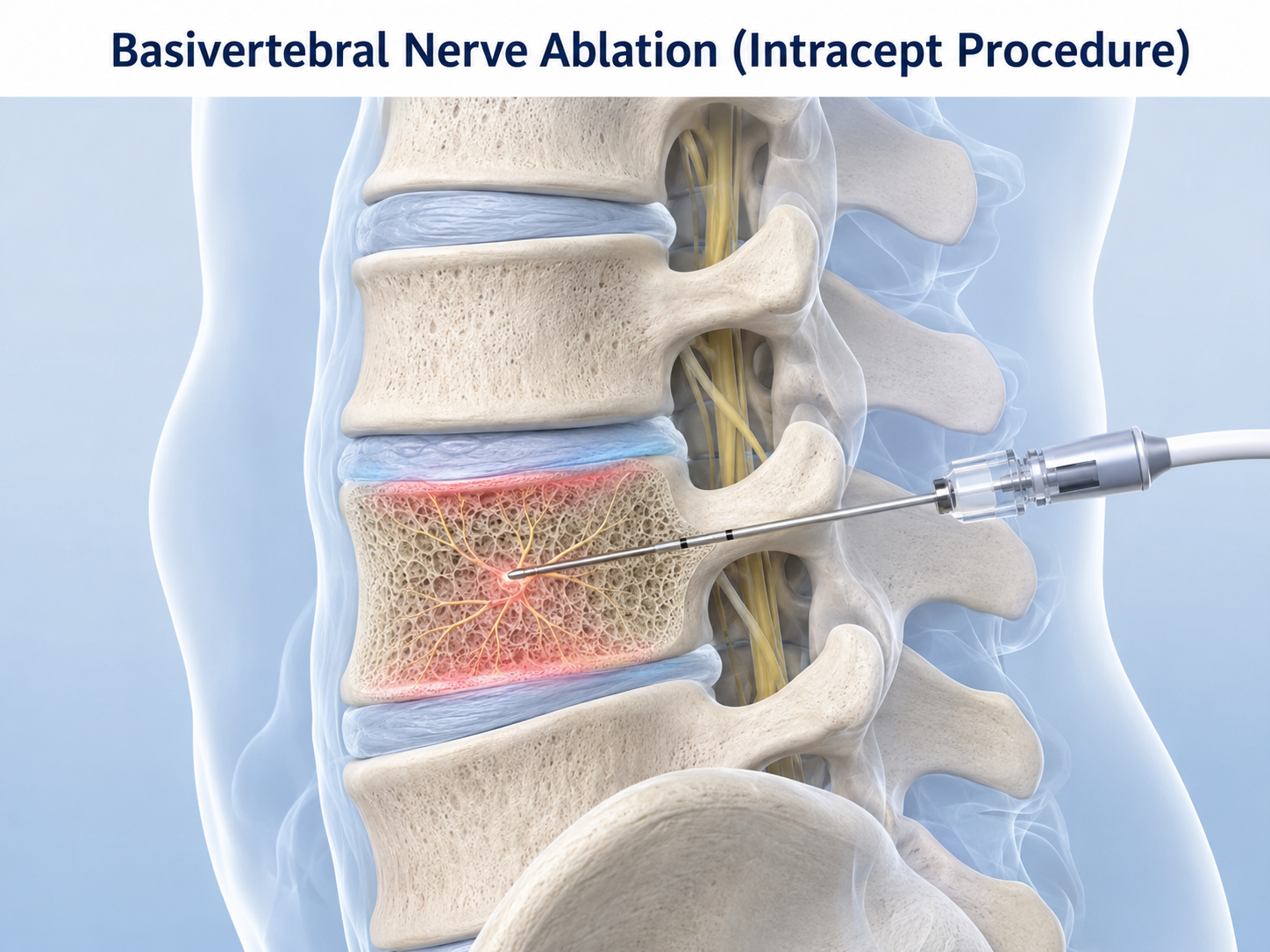
Basivertebral nerve ablation is a minimally invasive spine procedure used in selected patients with chronic vertebrogenic low back pain. “Vertebrogenic” means the pain is thought to come from damaged or inflamed vertebral endplates, which are the areas where the spinal bones meet the discs.
The Intracept Procedure is one form of basivertebral nerve ablation. It uses radiofrequency energy to target the basivertebral nerve inside the vertebral body. This nerve can carry pain signals from damaged endplates in the lower spine.
This procedure is not a general treatment for all back pain. It is considered only when the patient’s symptoms, physical examination, prior treatment history, and MRI findings suggest that the vertebral endplates are a likely pain source.
De Novo Brain & Spine evaluates adult patients in Stockbridge, Fayetteville, Atlanta, and surrounding communities to help determine whether back pain is more likely to come from vertebrogenic pain, nerve compression, spinal instability, arthritis, muscle strain, sacroiliac joint pain, or another cause.
Basivertebral nerve ablation is mainly used for selected cases of chronic vertebrogenic low back pain. It is not designed to treat every cause of low back pain.
Conditions or findings that may lead to consideration of this treatment include:
This treatment does not decompress nerves, remove a herniated disc, correct spinal instability, or fuse the spine.
Basivertebral nerve ablation may be considered when a patient has chronic low back pain that has continued despite appropriate non-surgical treatment and MRI findings suggest vertebral endplate inflammation or degeneration.
Patients being evaluated for this treatment often have pain centered in the lower back rather than pain that mainly travels down the leg. The pain may be worse with sitting, bending forward, lifting, or activity, but symptoms alone are not enough to confirm the diagnosis.
MRI findings are important. Modic changes are signal changes in the vertebral bone marrow near the disc and endplate. Modic type 1 changes often suggest inflammation or edema. Modic type 2 changes often suggest fatty marrow change related to degeneration.
Basivertebral nerve ablation is usually considered after conservative care has been tried. Conservative care may include medication, activity modification, physical therapy, home exercise, weight management when appropriate, and other non-surgical treatment options.
Doctors determine whether basivertebral nerve ablation may be appropriate by looking for a match between the patient’s symptoms, examination findings, imaging results, and prior treatment history.
Evaluation may include:
The diagnosis should not be based on MRI findings alone. Some people have degenerative changes on imaging that are not the main cause of their pain.
Basivertebral nerve ablation is performed using image guidance. A small access path is made into the vertebral body, and a radiofrequency probe is positioned near the basivertebral nerve.
Radiofrequency energy is then used to heat and ablate the nerve so it is less able to transmit pain signals from the vertebral endplate region. The procedure does not remove the disc, decompress the spinal canal, or place a spinal implant.
The number of vertebral levels treated depends on the patient’s MRI findings, symptoms, anatomy, and physician judgment. The exact setting, anesthesia plan, and procedural approach may vary.
The goal of basivertebral nerve ablation is to reduce pain signals from damaged vertebral endplates in carefully selected patients with vertebrogenic low back pain.
Potential benefits may include improvement in chronic low back pain and function when the basivertebral nerve is the correct pain target. Improvement is not guaranteed, and the procedure does not treat every cause of low back pain.
This treatment has important limitations. It does not treat spinal stenosis, sciatica from nerve compression, progressive weakness, spinal instability, deformity, fracture, infection, or tumor. It does not rebuild a damaged disc or reverse arthritis.
General risks may include pain at the procedure site, bleeding, infection, nerve irritation, fracture, incomplete symptom relief, or need for additional evaluation or treatment. Individual risks depend on the patient’s anatomy, medical history, bone quality, and overall health.
Treatment planning depends on the likely pain source. Basivertebral nerve ablation may be appropriate only when vertebrogenic pain is strongly suspected.
Other treatment options may include:
These treatments are not interchangeable. The best option depends on the diagnosis, imaging findings, neurologic examination, prior treatments, medical risks, and patient goals.
Recovery after basivertebral nerve ablation varies from patient to patient. It depends on the number of levels treated, the patient’s overall health, the severity of symptoms, and whether other spine problems are present.
Follow-up usually focuses on pain pattern, activity tolerance, neurologic symptoms, medication use, and whether additional treatment is needed. Some patients may continue physical therapy, home exercise, or other conservative care after the procedure.
Because this treatment targets pain signaling rather than removing a structural compression problem, patients should continue to report new or worsening neurologic symptoms promptly.
Seek emergency medical care or call 911 for new or worsening leg weakness, loss of bowel or bladder control, numbness in the groin or saddle area, difficulty walking, or sudden severe neurologic changes.
Urgent evaluation is also important for severe back pain after trauma, fever with severe back pain, unexplained weight loss with worsening pain, history of cancer with new severe back pain, or rapidly worsening leg symptoms.
Persistent low back pain that interferes with daily life should be evaluated by a medical professional, especially when symptoms continue despite conservative care.
Basivertebral nerve ablation is a minimally invasive procedure that uses radiofrequency energy to target the basivertebral nerve inside the vertebral body. It may be considered for selected patients with chronic vertebrogenic low back pain.
The Intracept Procedure is used for selected patients whose chronic low back pain is thought to come from damaged vertebral endplates. MRI findings, especially Modic type 1 or type 2 changes, are an important part of evaluation.
No. Basivertebral nerve ablation is not a general treatment for all low back pain. It is not designed to treat sciatica from nerve compression, spinal stenosis, instability, fracture, infection, tumor, or every type of degenerative disc disease.
Doctors look at the patient’s pain pattern, medical history, neurologic examination, MRI findings, prior treatments, and other possible pain sources. Modic changes on MRI may support the diagnosis, but imaging alone is not enough.
Not necessarily. The Intracept Procedure treats a specific pain pathway and does not decompress nerves or stabilize the spine. Patients with nerve compression, instability, deformity, or other structural problems may need different treatment.
Schedule a Consultation
Learn if this procedure is right for you.
Spinal cord stimulation is a neuromodulation treatment that may help selected patients manage chronic nerve-related pain signals.