Stroke
Evaluation and treatment planning for stroke, including ischemic and hemorrhagic stroke, urgent symptoms, vascular causes, and neurosurgical considerations.
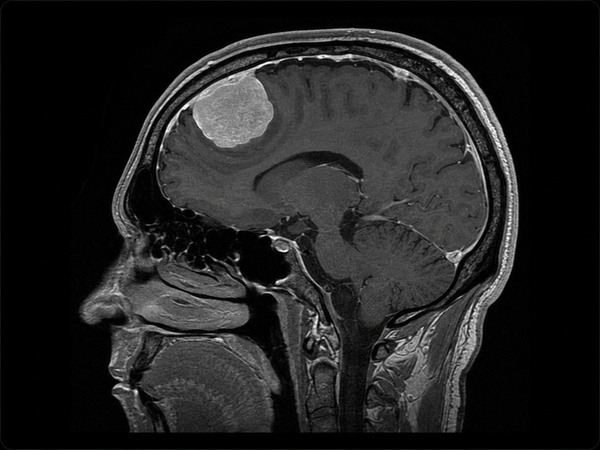
Meningioma is a tumor that develops from the meninges, the protective layers of tissue covering the brain and spinal cord. Many meningiomas are slow-growing and benign, but some can grow, press on nearby brain structures, involve the skull base, affect cranial nerves, or recur after treatment.
Meningiomas are commonly classified by CNS WHO grade. Grade 1 meningiomas are the most common and are usually lower-grade tumors. Grade 2 atypical meningiomas have a higher chance of recurrence. Grade 3 anaplastic meningiomas are malignant and more aggressive. The tumor’s grade, location, size, growth pattern, symptoms, and relationship to nearby brain structures all help guide treatment planning.
De Novo Brain & Spine evaluates adult patients with suspected or confirmed meningioma to help determine the appropriate next step. Evaluation may include neurological examination, brain MRI, CT imaging, review of prior scans, observation with repeat imaging, surgical consultation, pathology review, radiation oncology coordination, or additional specialty care when needed.
Meningioma symptoms depend on the tumor’s size, location, growth rate, and pressure on nearby brain, skull base, cranial nerve, or spinal structures. Some meningiomas are found incidentally on imaging and may not cause symptoms.
Common signs and symptoms may include:
Seek emergency medical care or call 911 for a first-time seizure, sudden weakness, sudden speech difficulty, sudden vision loss, severe confusion, loss of consciousness, or a rapidly worsening headache with vomiting or neurological changes.
Most meningiomas develop without a clearly known cause. A diagnosis of meningioma does not usually mean that the patient did something to cause the tumor.
Possible risk factors may include:
Doctors may also review tumor-specific features to guide treatment planning. These may include CNS WHO grade, tumor location, brain invasion, extent of resection, recurrence history, and selected molecular findings when appropriate.
These details help classify the meningioma and estimate clinical behavior, but they are not lifestyle causes.
Meningioma cannot be diagnosed by symptoms alone. Diagnosis usually requires medical history, neurological examination, and imaging. Tissue testing may be needed when surgery or biopsy is performed.
Common diagnostic steps may include:
The goal of diagnosis is to understand the tumor’s location, size, grade when known, relationship to nearby brain structures, and whether it is causing symptoms or growth over time.
Meningioma treatment depends on the tumor’s size, location, grade, growth pattern, symptoms, imaging findings, neurological examination, surgical risk, and the patient’s overall health. Not every meningioma requires immediate surgery.
Treatment options may include:
Surgery may be considered when a meningioma is growing, causing symptoms, pressing on important brain or nerve structures, causing seizures, affecting vision or hearing, or when tissue diagnosis is needed. The safest plan depends on the tumor’s anatomy and the patient’s individual condition.
Schedule a Consultation
Get an expert opinion about your condition.
Evaluation and treatment planning for recurrent brain tumors, when a previously treated brain tumor returns, grows, or progresses on follow-up imaging.
Evaluation and treatment planning for brain aneurysms, also called cerebral or intracranial aneurysms, including unruptured and ruptured aneurysms.