Craniotomy For Brain Tumor Resection
Craniotomy for brain tumor resection is brain surgery to remove as much tumor as safely appropriate for diagnosis or treatment.
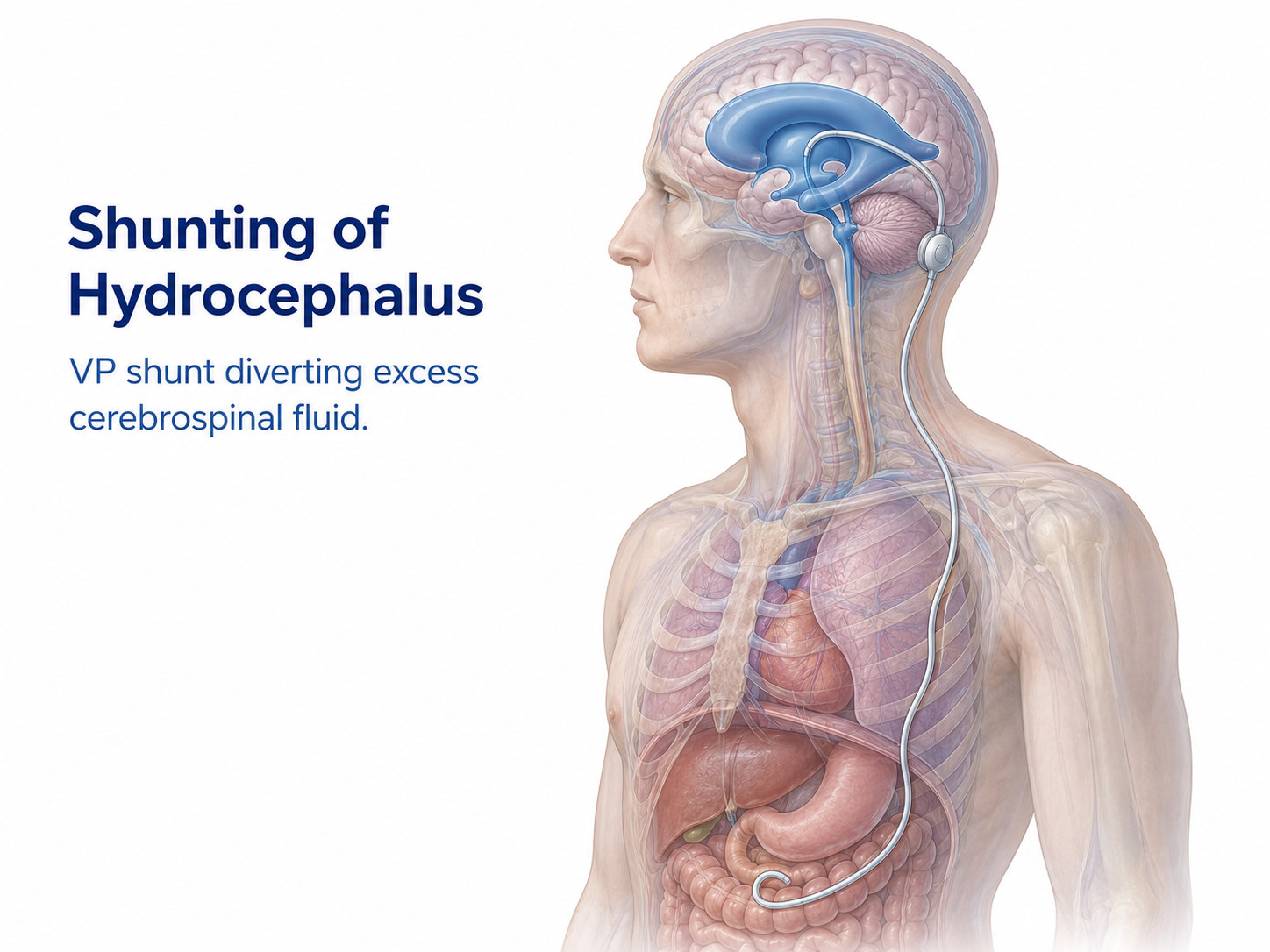
Shunting of hydrocephalus is a neurosurgical treatment that diverts excess cerebrospinal fluid, or CSF, away from the brain. CSF is the clear fluid that surrounds and cushions the brain and spinal cord.
Hydrocephalus occurs when CSF builds up in the ventricles, which are fluid-filled spaces inside the brain. This buildup can enlarge the ventricles and increase pressure on brain tissue.
A shunt is a thin flexible tube connected to a valve system. The shunt moves CSF from the brain to another part of the body, most often the abdomen, where the fluid can be absorbed. This is commonly called a ventriculoperitoneal shunt, or VP shunt.
Shunting may help control CSF buildup, but it does not necessarily cure the underlying cause of hydrocephalus. De Novo Brain & Spine evaluates adult patients in Stockbridge, Fayetteville, Atlanta, and surrounding communities to help determine whether shunting, endoscopic surgery, monitoring, or another treatment plan may be appropriate.
Shunting may be considered for selected patients with hydrocephalus or abnormal CSF buildup. It is not appropriate for every patient with enlarged ventricles or every patient with headaches, memory changes, or walking problems.
Conditions or situations that may lead to consideration of shunting include:
The treatment decision depends on the type of hydrocephalus, symptoms, imaging findings, neurologic examination, overall health, and whether CSF diversion is likely to help.
Shunting of hydrocephalus may be considered when CSF buildup is causing symptoms, pressure, ventricular enlargement, or neurologic decline. The urgency depends on the cause and speed of the CSF buildup.
Symptoms of hydrocephalus can vary. Some adults may develop headaches, nausea, vomiting, sleepiness, confusion, vision changes, balance problems, walking difficulty, bladder control problems, or memory changes. In normal pressure hydrocephalus, the classic symptom pattern may involve walking difficulty, cognitive changes, and urinary urgency or incontinence.
In some cases, hydrocephalus develops quickly after hemorrhage, tumor obstruction, trauma, infection, or surgery. These situations may require urgent hospital evaluation. In other cases, symptoms develop slowly and require careful outpatient testing to determine whether shunting is likely to help.
Shunting may be discussed when the symptoms, examination, imaging, and CSF testing suggest that diverting fluid could reduce pressure or improve the effects of CSF buildup. It should not be recommended from imaging alone.
Doctors determine whether shunting may be appropriate by reviewing the patient’s symptoms, neurologic examination, imaging findings, cause of hydrocephalus, medical history, and risks of surgery.
Evaluation may include:
The decision is individualized. Some patients with enlarged ventricles do not benefit from shunting if the symptoms are caused by another neurologic condition.
Shunt surgery is usually performed under anesthesia. In a ventriculoperitoneal shunt, a catheter is placed into a brain ventricle to drain excess CSF. The catheter is connected to a valve that helps control fluid flow.
Another catheter is tunneled under the skin from the head and neck down to the abdomen. The distal catheter drains CSF into the peritoneal cavity, the space around the abdominal organs, where the fluid can be absorbed.
Some shunts drain to other areas, such as the heart or pleural space near the lung, when a VP shunt is not appropriate. Some valves are programmable, meaning the drainage setting can be adjusted externally with a special device.
The exact shunt type, valve choice, catheter path, and surgical plan depend on the patient’s diagnosis, anatomy, prior surgery, infection risk, and surgeon judgment.
The main goal of shunting hydrocephalus is to divert excess CSF away from the brain so pressure or ventricular enlargement can be controlled.
Potential benefits may include improvement in symptoms related to CSF buildup, such as walking problems, headaches, vision symptoms, sleepiness, or cognitive changes, depending on the cause of hydrocephalus. Improvement is not guaranteed, and recovery varies.
Shunting has important limitations. It does not cure every cause of hydrocephalus. It does not reverse all brain injury. It does not guarantee improvement in walking, memory, bladder control, headaches, vision, or neurologic function.
Shunts also require long-term monitoring. A shunt can become blocked, infected, overdrain, underdrain, move out of position, or require revision surgery. Shunt problems can occur soon after surgery or years later.
General risks may include infection, bleeding, seizure, brain injury, shunt obstruction, shunt malfunction, overdrainage, underdrainage, abdominal complications, need for additional surgery, or persistent symptoms. Individual risks depend on the patient’s diagnosis, anatomy, prior surgery, medical condition, and shunt type.
Treatment planning depends on the type and cause of hydrocephalus. Shunting is one possible CSF diversion treatment, but it is not the only option.
Other options may include:
These treatments are not interchangeable. The best plan depends on the cause of hydrocephalus, whether CSF flow is blocked, how quickly symptoms are changing, the patient’s neurologic condition, and the risks and benefits of each option.
Recovery after shunting of hydrocephalus varies from person to person. It depends on the cause of hydrocephalus, the speed of symptom development, the patient’s neurologic status before surgery, overall health, and whether another brain condition is present.
Follow-up usually focuses on incision healing, neurologic symptoms, walking, cognition, headaches, vision, abdominal symptoms, and signs of shunt malfunction or infection. Imaging may be used to evaluate ventricular size and shunt position when needed.
Some patients may need valve adjustments, rehabilitation, repeat imaging, or additional specialist care. Patients with shunts should know the symptoms of shunt malfunction and should tell medical providers that they have a shunt.
Shunts may require lifelong monitoring. Even when symptoms improve, a shunt remains a medical device that can malfunction or become infected.
Seek emergency medical care or call 911 for severe headache, repeated vomiting, new seizure, sudden confusion, severe sleepiness, new weakness, trouble speaking, loss of consciousness, sudden vision changes, or rapid neurologic decline.
Patients with a shunt should seek urgent evaluation for symptoms that may suggest shunt malfunction or infection, such as worsening headache, nausea or vomiting, sleepiness, fever, redness or tenderness along the shunt path, abdominal pain, return of hydrocephalus symptoms, or new neurologic changes.
After shunt surgery, urgent evaluation is also important for fever, wound drainage, worsening incision redness, swelling around the shunt, clear fluid leakage, severe abdominal symptoms, or symptoms the surgical team specifically warned about.
Shunting of hydrocephalus is used to divert excess cerebrospinal fluid from the brain to another body area where it can be absorbed. It may be considered when CSF buildup causes pressure, enlarged ventricles, or neurologic symptoms.
A VP shunt is the most common type of shunt used for hydrocephalus. It drains CSF from the brain ventricles to the abdomen. Shunting of hydrocephalus is the broader treatment category.
A shunt can control CSF buildup, but it does not necessarily cure the underlying cause of hydrocephalus. Some patients need long-term shunt monitoring, valve adjustments, or revision surgery.
Doctors review symptoms, neurologic examination findings, MRI or CT imaging, the cause of hydrocephalus, prior treatment history, and medical risks. In selected normal pressure hydrocephalus cases, spinal tap or temporary CSF drainage testing may help predict response.
Possible shunt problem symptoms include worsening headache, nausea, vomiting, sleepiness, confusion, fever, redness or tenderness along the shunt path, abdominal pain, vision changes, seizure, or return of hydrocephalus symptoms.
Schedule a Consultation
Learn if this procedure is right for you.
Craniotomy for brain tumor resection is brain surgery to remove as much tumor as safely appropriate for diagnosis or treatment.
Endoscopic skull base surgery uses a small camera and specialized instruments to treat selected tumors or defects near the skull base.
Craniotomy for hematoma evacuation is brain surgery that removes a blood clot to reduce pressure on the brain when appropriate.