Metastatic Brain Tumors
Evaluation and treatment planning for metastatic brain tumors, also called brain metastases, when cancer spreads to the brain from another site.
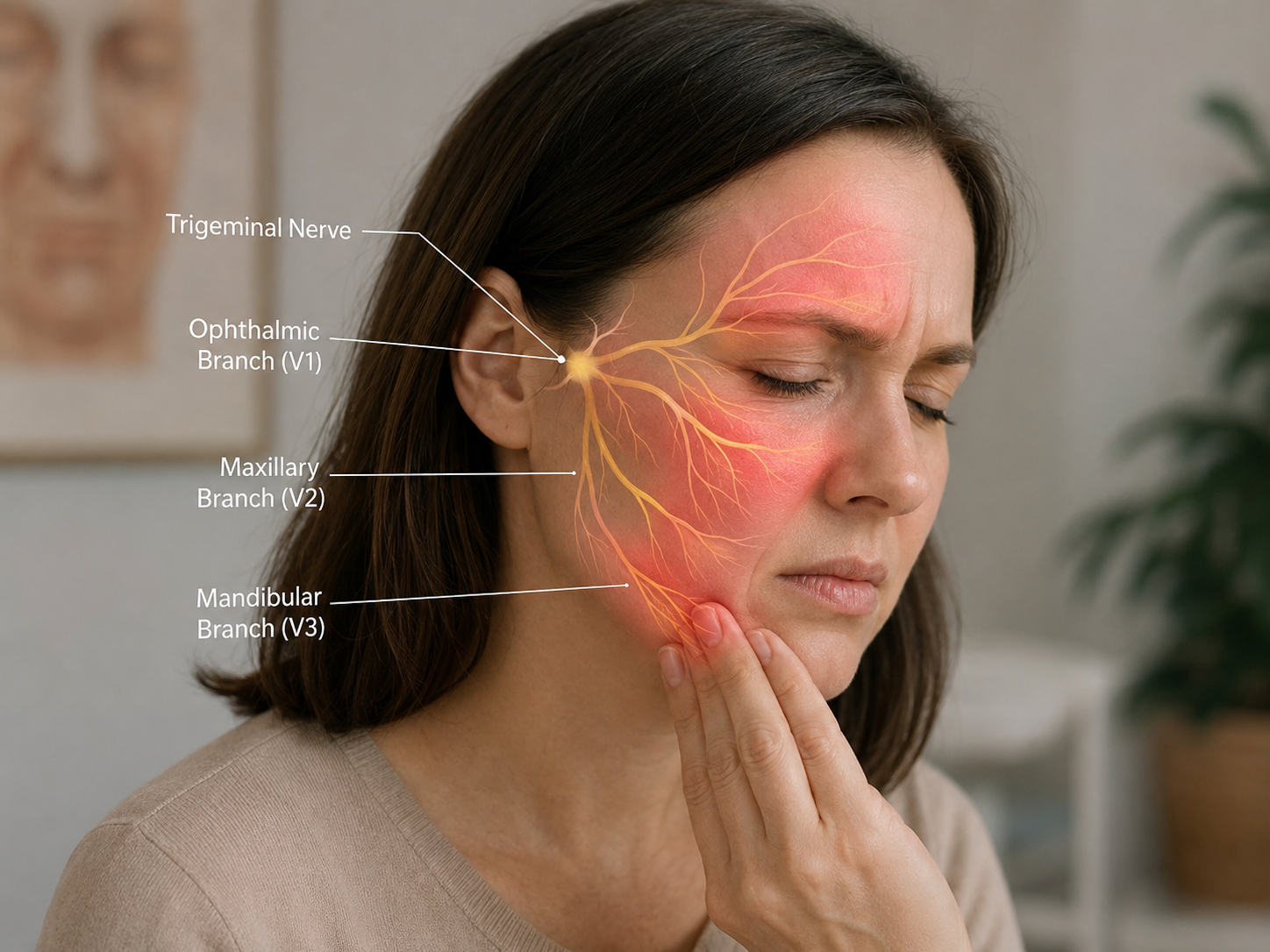
Trigeminal neuralgia is a cranial nerve pain condition involving the trigeminal nerve, also called cranial nerve V. This nerve carries sensation from the face, including the forehead, cheek, upper jaw, lower jaw, teeth, gums, and part of the scalp.
Trigeminal neuralgia can cause sudden episodes of severe, sharp, stabbing, shooting, or electric shock-like facial pain. The pain usually affects one side of the face and may involve one or more trigeminal nerve branches. These include the ophthalmic branch, maxillary branch, and mandibular branch.
De Novo Brain & Spine evaluates adult patients with suspected trigeminal neuralgia when symptoms suggest cranial nerve irritation, neurovascular compression, skull base disease, tumor, multiple sclerosis, prior nerve injury, or facial pain that has not been explained by dental, sinus, jaw, or primary headache conditions.
Trigeminal neuralgia symptoms depend on which branch of the trigeminal nerve is involved, the pain trigger, and whether the condition is classical, secondary, or idiopathic.
Common signs and symptoms may include:
Seek urgent medical evaluation for facial pain with new numbness, facial weakness, double vision, trouble swallowing, hearing changes, severe headache, fever, facial swelling, confusion, or rapidly worsening symptoms. Seek emergency medical care or call 911 for sudden facial drooping, arm weakness, speech difficulty, sudden vision loss, loss of consciousness, or other stroke-like symptoms.
Trigeminal neuralgia occurs when the trigeminal nerve becomes irritated or affected along its pathway. In many classical cases, a nearby blood vessel contacts or compresses the trigeminal nerve near the brainstem. This is called neurovascular compression.
Possible causes and related factors may include:
These causes and related factors do not mean every patient has a tumor or serious structural condition. Treatment planning depends on the pain pattern, neurological examination, imaging findings, response to medication, and whether another dental, sinus, jaw, headache, or neurological condition is identified.
Trigeminal neuralgia is diagnosed through careful history, physical examination, neurological examination, and targeted testing when appropriate. The pain pattern and triggers are very important because trigeminal neuralgia can be confused with dental disease, TMJ disorder, sinus disease, migraine, cluster headache, or other facial pain conditions.
Common diagnostic steps may include:
The goal of diagnosis is to determine whether symptoms fit trigeminal neuralgia, identify whether a structural cause is present, and distinguish trigeminal neuralgia from painful trigeminal neuropathy, dental disease, TMJ disorder, sinus disease, migraine, or other facial pain conditions.
Trigeminal neuralgia treatment depends on the pain pattern, severity, triggers, neurological examination, imaging findings, suspected cause, prior medication response, surgical risk, and overall health. Not every patient needs surgery.
Treatment options may include:
Neurosurgical treatment is not appropriate for every patient with trigeminal neuralgia. Neurosurgical evaluation may be considered when symptoms suggest neurovascular compression, skull base disease, tumor, structural nerve compression, or facial pain that remains severe despite appropriate medical treatment. Patients with trigeminal neuralgia may also need evaluation for related facial pain when symptoms overlap with dental, sinus, jaw, headache, or other nerve-related conditions.
Schedule a Consultation
Get an expert opinion about your condition.
Evaluation and treatment planning for metastatic brain tumors, also called brain metastases, when cancer spreads to the brain from another site.
Evaluation and treatment planning for pituitary tumors that may affect hormone function, vision, headaches, and nearby skull base structures.
Evaluation and treatment planning for ventricular tumors, brain tumors located near cerebrospinal fluid pathways that may cause hydrocephalus or neurological symptoms.